Introduction
Clostridium difficile (C.difficile) is an anaerobic, spore-forming bacillus causing antibiotic-associated diarrhea & pseudomembranous colitis. It colonizes 2% of healthy people & 3-26% of individuals in a hospital setting.1, 2 The spores can live up to 6 months on surfaces in the hospital.3 A hospitalized patient acquire infection from hands of health care worker or the hospital environment and predisposing factors such as antibiotic use, prolonged hospitalization, gastrointestinal surgery, and advanced age can lead to C. difficile infection(CDI).4 This colonization becomes clinically significant when the strains produce toxins . C. difficile pathogenesis is mainly due to production of toxin A; TcdA & toxin B: TcdB. In addition some strains produce another toxin is Binary toxin:CDT made up of CDTa(enzymatic component) & CDTb(binding component).5 Presence of CDT in addition to TcdA & TcdB is associated with severe disease & higher mortality.6 A more virulent strain, BI/NAP1/027 reported first time from China in 2012 has been linked to severe disease and reported worldwide later on.7, 8, 9 Detection of these toxigenic strains in stool is necessary to initiate early therapy & to implement infection control measures. Various laboratory tests such as stool culture, CCNA (culture cytotoxicity neutralization assays), GDH (Glutamate dehydrogenase) assays, EIA (Enzyme immunoassays) for toxin detection, and NAAT(nucleic acid amplification) tests available for the diagnosis of CDI.5 Culture & CCNA have longer turnaround time. American society for microbiology & IDSA (Infectious Disease Society of America) has recommended that toxin detection by EIA for diagnosis of CDI is insensitive & not recommended as standalone test.10, 11 It is recommended to use NAAT alone or a multistep algorithm for testing (GDH+TOXIN or TOXIN+NAAT or GDH+TOXIN arbitrated by NAAT).10, 11 Incidence of C. difficile associated diarrhea (CDAD) has been observed from 7 to 30% in Asian countries.12 A meta-analysis study reported 8.9% mortality & 14.8% nosocomial diarrhea cases due to CDAD.12 Though some Indian studies have reported the epidemiology, prevalence, risk factors & molecular characterization of CDI.13, 14, 15, 16 The problem is underestimated & data on CDI is still lacking in India. Keeping this in mind the study was planned to determine the positivity of CDI by using multiple tests including GDH plus toxin assay and NAAT testing.
Materials and Methods
This is an observational study, approved by the Institutional Ethics committee (IEC), conducted in the Department of Microbiology, Dayanand Medical College and Hospital, Ludhiana from February 2019– May 2020. All the stool samples received in the department during this period from the suspected patients of CDI included in the study.
Specimen
Total of 1429 of freshly passed stool samples received and processed immediately in the lab. The samples were tested by rapid ICT (Vitassay) for GDH Ag and toxin A & toxin B or by PCR (cepheid) for toxigenic gene.
Immunochromatographic test (Vitassay)
It is a rapid one step immunochromatographic test (ICT) for the qualitative detection of C. difficile GDH Ag, toxin A & B in human stool samples. The test line zones of the nitrocellulose membrane are pre-coated with monoclonal antibodies against GDH, toxin A & toxin B. During the process, the sample reacts with the antibodies, forming conjugates. The mixture moves upward on the membrane by capillary action. If the sample is positive, antibodies present on the membrane (test line) capture the conjugate complex and a corresponding red line will be visible. The presence of this green line in the control zone (IC) indicates that sufficient volume is added; proper flow is obtained and serves as an internal control for the reagents. Test procedure was done as per kit protocol. Briefly, Sample was added to the sample dilution vial and shook vigorously to obtain a good sample dilution and placed inside the multiplex tube. The cap of the multiplex tube was screwed tightly. The bottom of the vial for sample dilution breaks and the diluents & sample solution reaches the sample zone of the strip. The multiplex tube was kept vertically on a flat surface and the results were read at 10 minutes.
GeneXpert C. difficile PCR Assay
The GeneXpert C. difficile Assay (Cepheid) is qualitative automated real-time PCR test for the rapid identification & detection of Toxin producing C. difficile, It detects C. difficile toxin B gene (tcdB), binary toxin gene (cdt) & BI/NAP1/027 strain. Test procedure was performed according to the manufacturer’s recommendations. The specimen was vortexed at high speed for 15 seconds before a sterile dry swab was dipped into the stool for testing. Excess stool was removed and the swab was placed into a vial containing the sample reagent (guanidinium thiocyanate and surfactants). The swab’s stem was then broken off after lifting it a few millimeters so that the cap could be closed tightly before it was vortexed at high speed for 10 seconds. Using a clean transfer pipette, the entire content of the tube was transferred into the S-chamber of the disposable GeneXpert C. difficile fluid cartridge, which was then placed into the GeneXpert Dx System instrument
for analysis. The results were determined by the GeneXpert Dx System from measured fluorescent signals and embedded calculated algorithms. The invalid result was reported when sample processing control was failed; indicating that the sample was not properly processed or PCR was inhibited.
Results
A total of 1429 stool samples received in the laboratory for C.difficile testing. Out of these 1415 samples were tested by ICT for presence of GDH Ag/Toxin A/B, 48 samples were tested by PCR & 34 samples were tested by both ICT & PCR.(Figure 1)
Total 188(13.15%) samples received from 165 patients 94(57%) male patients and 71(43%) female patients, from various age groups were found positive for CDI.(Table 1) More than one samples were received from 15 patients.CDI positivity of patients is shown in Table 2
Out of all 187(13.21%) samples were found positive by ICT. GDH Ag was detected in 184(13%) samples & 97 (6.8%) samples were found positive for toxin by ICT &PCR. Among 1228(86.78%) GDH Ag negative samples, 3(0.24%) were found positive for toxin A/B. (Table 3) A total of 48(14 only PCR + 34 ICT & PCR) samples were tested by PCR. (Figure 1) Among these TcdB gene was detected in 5(10.41%) samples. Out of 5 PCR positive samples, one sample was tested only by PCR & 4 samples were tested by ICT also. Out of these 4, three samples showed results as only GDH positive & one sample was found positive for GDH Ag as well as for toxin A & toxin B in the ICT test.
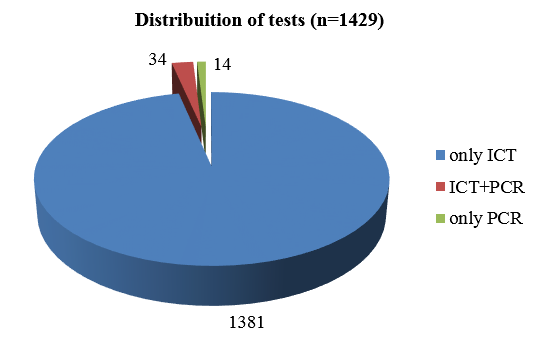
Table 1
Age wise distribution of the CDI positive patients
| Age group | No. of cases | Percentage |
| 0-9 | 1 | 0.6% |
| 10-19 | 6 | 3.6% |
| 20-29 | 19 | 11.5% |
| 30-39 | 22 | 13.4% |
| 40-49 | 25 | 15.1% |
| 50-59 | 34 | 20.6% |
| 60-69 | 29 | 17.5% |
| 70-79 | 23 | 13.9% |
| 80-89 | 5 | 3.0% |
| 90-100 | 1 | 0.6% |
| Total | 165 | 100.0% |
Table 2
GDH & Toxin positivity1 according to gender of the patients (n=165)
.
Discussion
Various studies have shown incidence of CDAD in hospitalized patients ranging from 3-29%. 17, 18 Positivity of toxigenic C.difficile infection in our study was found to be around 7%. The positivity rate in our hospital is not very high as compare to other studies, could be due to stringent infection control practices followed by infection control team & treatment is being given according to antibiotic policy.
Old age (>60 years) is an important risk factor for C.difficile infection as 10% of them are colonizers.19 In our study most of the positive patients were between 30-80 years of age group & maximum (21%) were between 50-60 years of age similar to L.segar et al who reported maximum positive patients between 50-60 years.17 Yanyan Xiao et al reported 55.3 years of average age of the patients in their study. 20
In the current study, no significant gender difference was observed in toxigenic CDI. Though it was found slightly more in males (16.3%) as compared to females (15.6%). Other Indian studies have reported varied mean age and male female ratio. 21 In the study 13% of samples were found GDH positive. GDH is the antigen present in toxigenic as well as non toxigenic strains of C.difficile. This test can be used as screening test due to it’s high sensitivity. Cheng et al reported 32.2% positivity by GDH assay. 22 Their study reported, the sensitivity, specificity, PPV and NPV of VIDAS GDH assay as 100.0%, 92.8%, 83.6% and 100.0%, respectively as compare to routine C. difficile culture. Other studies have reported sensitivity of 85-95% and specificity of 89-99%. 23, 24 Among the GDH positive samples approximately half of them were found negative for toxin. Out of total, only 7% were detected positive for toxin. Among the toxin producing samples 29% were positive for toxin A only, 4.3% for toxin B alone & 66.7% were found positive for both the toxins. Although, most easy & rapid methods for detection of toxigenic C.difficile strains are toxin immunoassays but Toxin assays should not be used as standalone for diagnosis as toxins may not present at detectable level in feces of some patients. There is a probability of getting false negative results due to unstable nature of the toxins, degradation may occur during transportation at room temperature. We had experience in the laboratory; negative samples from patients with high clinical suspicion turn out to be positive when tested with fresh repeat sample. Another limiting factor for these assays are their low sensitivity (52-75%), however, they have good specificity ranging from 96-98%.25 Senok et al reported 20.5% positivity by immunoassay, another study Reported 36.8% toxin positivity in GDH positive samples by immunoassay. 26, 27 In our study around 52% of GDH positive samples showed the presence of toxin.
High cost of the test was a limiting factor for PCR assay in our study. We could not receive samples for all the GDH positive samples. Only 3.5% samples were tested by PCR & 29% of them were tested by PCR alone. Among all PCR tested samples 10.4% were found positive for toxin B. All the samples were negative for binary toxin, Tcdc & presumptive 027 ribotype. A study from Saudi Arabia reported 52.6% toxin positivity by GeneXpert in GDH positive samples. 27 Various studies reported sensitivity & specificity of Gene xpert as 90-100%, 92.9-98.6% respectively. 28 Three, only GDH Ag positive samples were found positive for tcdB gene (toxin B) in PCR test. In these samples toxin detection was missed by immunoassay. These samples showed clinical correlation & response to treatment for C.dffiicile associated diarrhea. On the other hand NAAT do not detect active toxin production. It can show positive result in asymptomatic patients which can lead to over diagnosis of the infection.29 Polage et al. showed less severe symptoms in PCR positive but immunoassay negative as compare to both test positive patients.30 Another limitation of GeneXpert PCR it does not detect gene for toxinA production. In contrast to other studies, out of all positive samples 14% were due to only toxin A production in our study.5 More studies need to be done to increase the awareness among clinicians to prevent the spread of C.difficile associated diarrhea & to improve the diagnostics. Correct & timely diagnosis & stringent infection control practices are the mainstay to combat this worrisome nosocomial disease.
Conclusions
To improve the diagnosis of C.difficile associated diarrhea a multi step algorithm for testings is required. Test done with freshly collected sample can improve the sensitivity of immunoassay. High cost of multistep testing and NAAT testing is still a hurdle for diagnosis of C.difficile in the developing countries.