Introduction
Hepatitis is a universal concept that mean inflammation of the liver and infection with 1 of the 5 viruses called hepatitis A, B, C, D and E viruses is the almost common cause. The 5 viral cause’s hepatitis-B infection is the worldly almost common hepatic infection, which is cause by hepatitis-B (HBV). HBV is a DNA virus. It is 42–47 nm in diameter and enters the liver through with blood stream.1 Early Hepatitis-B envelope seroconversion in the immune response consent phase has is given away to point out an approving result in the usual way of chronic liver HBV infection.2 In typical cases of acute Hepatitis detection HBeAg has small value. However in chronic infection HBeAg is a main marker of viral duplication infection and continuing liver injury.3 HIV, HBV, and HCV are three almost universal chronic viral infections all over the world. They contribute to similar transmission route as well as sexual intercourse, mother-to-child transmission and inject drug usage.4, 5
Aim & Objective
Study of occurrence of HBeAg among Hepatitis- B surface antigen positive cases; 1. Identification of Hepatitis B Surface Antigen positive cases; 2. Occurrence of HBeAg among Hepatitis- B surface antigen positive cases.
Inclusion criteria
Age >18 years will be included of either sex.
Cases with signs and symptoms suggestive of Hepatitis attending OPD & IPD.
Patients reactive with Hepatitis B Surface antigen will be included.
Exclusion criteria
Known Hepatitis-B vaccinated patients.
Cases with hepatic disorders.
Other diagnosed causes of jaundice like Hepatitis-A, Hepatitis-C, Cholelithiasis etc.
Materials and Methods
The research design was attached in serology section of microbiology department, Teerthanker Mahaveer hospital (Moradabad), from September 2018 to December 2019. Total 106, HBeAg suspected cases were interpreted in this study. Patients of all age grouping with a history of body temperature, sickness, pale yellow skin, or liver cancer were involved in this study. The sample was transported to designated place for processing. 5ml blood was collected from anterior cubital vein by Venipuncture from recruited patient. Samples were collected after proper consent and aseptic precautions. Then every blood sample was transfer overhead a tagged tube plane vial.
Observation & Result
The Study was conducted in Department of Microbiology, Teerthanker Mahaveer hospital. Blood sample from 106 HBsAg positive patients including both male and female were collected from various department of the Hospital for the analysis purpose. Out of them, 38(35.85%) cases were HBeAg Reactive and 68 (64.15%) cases were HBeAg non Reactive. A total of 106 HBsAg positive cases were selected in this study as per the inclusion and exclusion criteria.
Table 1
The HBeAg distribution in all HBsAg positive cases
|
S. No. |
Test |
Number of patients |
Percentage (%) |
|
1. |
HBeAg reactive |
38 |
35.85% |
|
2. |
HBeAg Non-reactive |
68 |
64.15% |
|
|
Total |
106 |
100% |
Out of the total cases, 38 (35.85%) cases were HBeAg reactive and 68 (64.15%) cases were non-reactive as shown in Table 1.
Table 2
Sex wise distribution of HBeAg reactive cases
|
S.No. |
Sex |
HBeAg Reactive |
|
1. |
Male |
29 |
|
2. |
Female |
9 |
|
|
Total |
38 |
Shows out of 38 reactive cases of HBeAg 29 were male and 9 were female having HBeAg infection.
Figure 1
Age and Gender wise distribution in Male and Female different age group of HBeAg Reactive and Non-reactive cases.
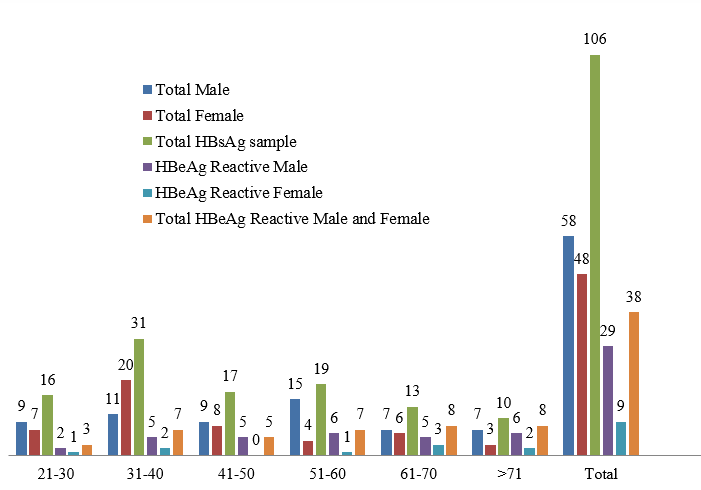
Out of 106 HBsAg reactive cases, 38 cases were reactive for HBeAg and 68 cases were non-reactive.
Age 21-30 years reactive cases 2 male & 1 female, 31-40 years reactive cases 5 male & 2 female, 41-50 years reactive cases only 5 males, 51-60 years reactive cases 6 male & 1 female, 61-70 years reactive cases 5 male & 3 female and above 70 years reactive cases 6 male & 2 female cases.
Figure 2
Showing total 106 patients were selected in this study. The total OPD & IPD distribution HBeAg Reactive cases
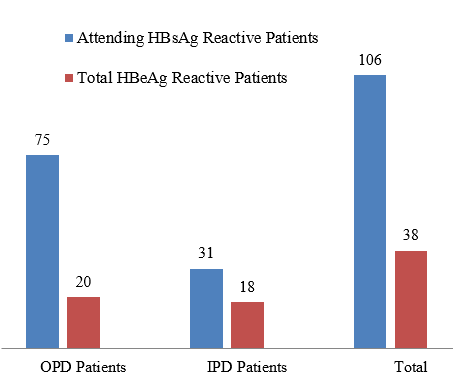
Showing:-Out of them, 38 HBeAg positive cases. The distribution in these cases of 20 cases was OPD and 18 cases were IPD.
Discussion
HBV is a DNA virus, which is responsible for 1 million patients die every year geographically. HBV remnants a community health effect within the globe almost in increasing countries. Work-related exposure of hospital worker to contaminated blood and blood material remain a main risk issue. Health care workers are at risk of acquiring HBV disease and as well transmit it to new person in the route of their scientific and lab duty. 6 Reactive HBsAg test suggest infection but it doesnot give any information regarding the infectivity stage of the virus. 7
Hepatitis-B core Antigen-HBcAg is a viral hepatitis-B protein. It is a sign of reactive viral reproduction and the patient infected with Hepatitis-B can expect transmitting the infection into the person. 8 Hepatitis-B envelope Antigen- HBeAg is an antigen that can be located between the nucleo capsid heart of the icosahedral and the outermost layer of the HBV lipid envelope. 9 All the same HBeAg is measured non-particulate and secretory. At the same time as together HBeAg and HBcAg are complete from the same reading border. HBeAg is unseen and accumulates in blood and serum and can be tested as an immunologically separate soluble antigen. 10 This antigen is a protein particle starting the HBV that circulate in contaminated patient’s blood as the virus part is vigorously replicating. The presence of HBeAg suggests that the patient is highly infective and can transmit the disease to new people by sexual transmission or by vertical transmission. 11 HBeAg are little polypeptide so as to exists in a without charge form in the blood serum test of persons during the early on stage of hepatitis-B disease, almost immediately later HBsAg becomes visible. Serum levels of HBeAg and HBsAg increase the time of viral replication. 12 Hepatitis-B viruses are the major etiologic factors in alcoholic and non alcoholic fatty liver disease. Chronic hepatitis-B infections are the leading causes of cirrhosis and hepatocellular carcinoma worldwide. 13 The prevalence of HBV infection among patients of Teerthanker Mahaveer medical college and hospital laboratory science U.P. India was presented in the current report. In this study, out of total 106 cases, 38 cases were HBeAg reactive and 68 cases were HBeAg non-reactive. Our study is similar to study by Madeddu G et al where 113 cases were HBeAg reactive. The male predominance was more with 61% (68 males) compared to females by 39% (45females). Our study differs from study of Hsuan W et al. 14 HBeAg reactive cases have high HBV DNA levels. However this test is costly compared to detection of HBeAg and hence HBV DNA can be suggested to those patients who are HBeAg reactive. Also chronic HBV infection can go through various phases that can affect therapeutic consideration. HBeAg status along with liver function test helps in assessing the stage of the disease and also provide information regarding the need for liver biopsy and treatment strategy. If HBeAg was present in the initial stages of the disease and becomes negative during the treatment of the patient suggesting seroconversion, this indicates that the patient is responding to the treatment protocol. The present study demonstrates the common symptoms found in these cases were nausea 92%, joint pain 76%, headache 61%, jaundice 79% and vomiting 74%. This is in agreement with some earlier studies like Bruix J et al. Showed in their study the most common symptoms found was fever 100%, abdominal pain 100% and loss of appetite 100%. In contrasts, few investigators showed various results. Dusheiko G et al showed in their study HBV was the major clinical presentation then fever and abdominal were also common presenting features. Hence we can safely say that the clinical picture observed in the current study is quite similar to any other febrile illness like other virus disease and hence it can be considered as a tool for diagnosis. 15 In our study 38 patients were infected with HBeAg. The male predominance was more with 29 (% male) compared to females by 9(% females). Our study is similar to study by Mustafa el et alwhere 245 cases were HBeAg reactive, 120(49%) were males while 125(51%) were females. Our study differs from study of Alo MN et al. Presence of HBeAg and absence of HBe antibody (anti-HBe) usually indicate active HBV replication and high infectivity. Absence of HBeAg with appearance of anti-HBe is consistent with loss of HBV infectivity. Although resolution of chronic HBV infection generally follows the appearance of anti-HBe, the HBV carrier state may persist.16 Several antiviral medications — including entecavir (Baraclude), tenofovir (Viread), lamivudine (Epivir), adefovir (Hepsera) and telbivudine (Tyzeka) — can help fight the virus and slow its ability to damage the liver.Interferon injections-interferon Alfa-a(Intron A)is a man-made version of a substance produced by the body to fight infection. Alcohol may be harmful and aggravate certain conditions.17
The infectivity and chronicity in Hepatitis B positive patients
In HBV carriers and patients with chronic hepatitis B, positive HBeAg results usually indicate presence of active HBV replication and high infectivity. A negative HBeAg result indicates very minimal or no HBV replication. Positive anti-HBe results indicate inactivity anti-HBe results in the presence of detectable HBV DNA in serum also indicate active viral replication in these patients.[18] Out of 106 active person HBsAg, 58(%) were male as well as 48(%) were female. Out of 58 males, 29 (%) were haveHBeAg positive and out of 48 females, 9(%) were having HBeAg positive. Our study is similar to study by Madeddu G et al who found that males were infected more than females in HBeAg positive cases. Our study is similar to study by Mustafa EL et al who found that males were 49% and female were 51%. Our study differs from study of Alo MN et al. In our report, the main age wise of HBV reactive person along with both sexes male and female cause through HBeAg was 51-60 year. Our study is similar to the study Madeddu G et al and Mustafa EL et al who observed same age group 51-60 year was affected by HBeAg infection. In this sample HBeAg was highest among the age group of 51-60 yrs. This is equivalent to the report by Madeddu G et al which found HBeAg to be high person infected between both sexes of 45-60 yrs age group in Italy. The age of acquire the illness is single of the determinants of the frequency rates of HBeAg.
Conclusion
The result of our study put up valuable information and connection in HBeAg positive cases.
In this little sample size 106 analysis of the patients at Uttar Pradesh Teerthanker Mahaveer Medical College, the prevalence of HBeAg (positive results) in the department of medical microbiology, while the negative result is 68(64%). Males 29(76%) were more affected by the HBV (HBeAg) infection as compare to Female 9(24%). An important preventive measure is the screening for HBV in blood donors. Hepatitis-B related chronic liver disease and hepatocellular carcinoma are best prevented by universal childhood immunization. In non-infected people, HBV infection can be avoided by HBV vaccination. Injections Sequence 3 at 0, 1 and 6 months. In over 90% of recipients vaccination is successful. Surveillance is required to monitor for disease and HBV variants. The prevalence of HBV in the patients attending Teerthanker Mahaveer hospital was very low in compare to the general population in India. The prevalence of HBV is very high in rural people with compare to urban people. Rural people are not aware about vaccination due to lack of education so the whole nation and vaccination programmed should be implemented properly by the government against HBV infection.
Ordinary Precautions
Universal precautions are called occasionally.
Using it to sever the infection chain.
Blood and body fluids are used to transmit diseases.
Provide sufficient facilities and equipment for hand washing.
Ensure that the work environment is safe and healthy.
Dispose of infectious waste correctly.
Cover up any open wounds or sores before proceeding.
Acknowledgment
I would like to thanks entire Microbiology department, TMMC & RC for their guidance and cooperative behavior.